Tannins are "sticky." The hydroxyl groups (-OH) on theaflavins and EGCG coordinate with metal ions, forming insoluble chelate complexes that you excrete rather than absorb. This is why drinking strong black tea with a steak causes iron-deficiency anemia, but drinking it after eating tuna prevents mercury poisoning.
Chelation is dose-dependent, metal-specific, and timing-sensitive. This guide explains the chemistry, clinical applications, and how to weaponize tea's binding power (or avoid it).
Chelation vs. Absorption: The Critical Difference
Chelation PREVENTS absorption (metals bound in your intestines never enter bloodstream). Absorption is what happens when metals DO cross the gut barrier. Tea chelates metals IN THE GUT (good for detox, bad for nutrition). It does NOT chelate metals already IN YOUR BLOOD (that requires IV EDTA therapy). Timing is everything.
The Chemistry of Chelation
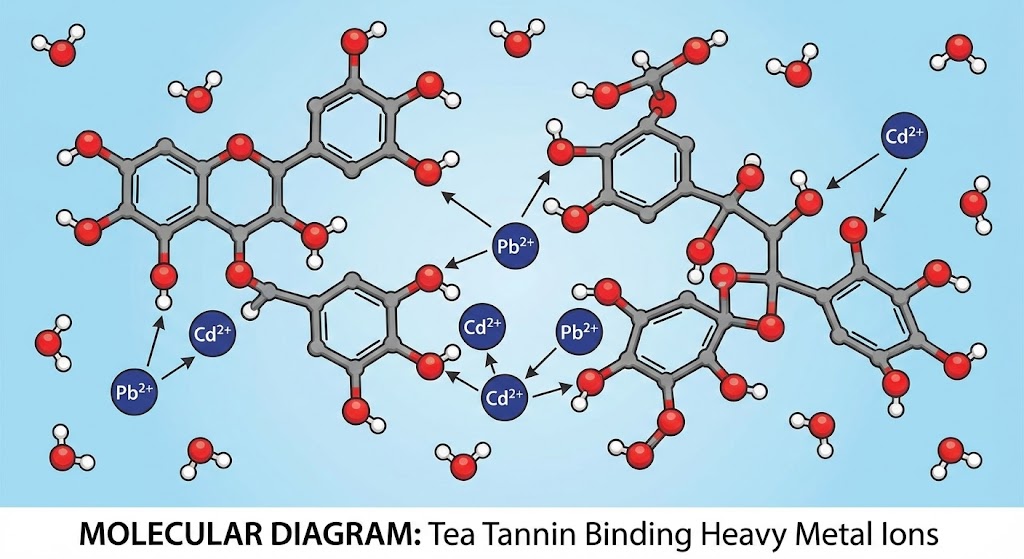
A chelate (from Greek "chele" = claw) is a metal ion surrounded by organic molecules via coordinate covalent bonds. Tea polyphenols have multiple hydroxyl groups that "grab" metal ions in a cage-like structure. The resulting complex is too large to pass through intestinal walls.
The Binding Reaction (Iron Example)
Fe²⁺ + 2(Tannin-OH) → Fe(Tannin)₂ (insoluble precipitate)
This reaction occurs in your stomach (pH 2-3) and small intestine (pH 6-7). The iron-tannin complex passes through your digestive tract unabsorbed and exits in feces (which turn dark/black from iron sulfide).
Metal-Specific Binding Strength
| Metal Ion | Formation Constant (log K) | Binding Strength | Health Context | Tea Strategy |
|---|---|---|---|---|
| Lead (Pb²⁺) | 10.2 | STRONGEST | Neurotoxic, no safe level | Drink tea after lead exposure (paint, soil) |
| Mercury (Hg²⁺) | 8.7 | STRONG | Bioaccumulates in fish | Drink tea 1-2 hours after seafood |
| Copper (Cu²⁺) | 7.9 | MODERATE | Essential trace mineral | No intervention needed (adequate intake) |
| Iron (Fe²⁺) | 6.4 | MODERATE | Anemia vs. hemochromatosis | Avoid tea with meals if anemic |
| Zinc (Zn²⁺) | 5.1 | WEAK | Immune function | Minimal interference (separate by 1 hour) |
| Calcium (Ca²⁺) | 3.2 | VERY WEAK | Bone health | Tea does NOT deplete calcium (myth) |
Key Insight: Tea preferentially binds toxic metals (lead, mercury) over essential minerals (zinc, calcium). This is why tea is protective against environmental toxins but risky for iron-deficient populations.
The Iron Paradox: Anemia vs. Hemochromatosis
How Tea Causes Anemia
Non-heme iron (from plants, grains, supplements) requires vitamin C for absorption. Tannins compete by forming Fe(tannin) complexes, reducing bioavailability by 70-80%. One cup of tea with a meal can drop iron absorption from 10% to 2%. This seemingly small difference becomes clinically significant over time—a woman absorbing 2% instead of 10% from a 15mg dietary iron intake loses 1.2mg per day, totaling 36mg monthly. For menstruating women already losing 15-30mg monthly through blood loss, this tips the balance into deficiency.
The populations most vulnerable to tea-induced anemia include menstruating women who lose 15-30mg iron monthly through blood, creating a narrow margin between intake and loss. Vegans and vegetarians rely entirely on non-heme iron from plants (beans, spinach, fortified grains), which is already poorly absorbed (5-10% baseline) compared to heme iron from meat (15-35% absorption). When tea tannins interfere, absorption drops to 1-3%, making it nearly impossible to meet iron requirements through diet alone. Pregnant women require 27mg iron daily (vs. 18mg for non-pregnant women) to support fetal development and placental blood volume expansion—tea consumption during pregnancy can trigger maternal anemia and increase risk of low birth weight. Finally, children in growth spurts have elevated iron demands for rapid tissue synthesis and blood volume expansion; chronic tea consumption during these windows can stunt growth and impair cognitive development.
The mechanism is simple but insidious: polyphenolic gallotannins (especially theaflavins in black tea) chelate ferrous iron (Fe²⁺) in the stomach and small intestine before it can bind to transferrin for absorption. The resulting Fe(tannin)₂ complex is too large and nonpolar to cross intestinal epithelium, so it passes through the digestive tract unabsorbed and exits in feces. The formation constant (log K = 6.4) indicates moderate binding strength—strong enough to block absorption, but weaker than lead or mercury chelation.
The Anemia Prevention Protocol
- Drink tea between meals, not with meals (2-hour gap minimum)
- Consume vitamin C-rich foods (citrus, bell peppers) to counteract tannins
- Choose heme iron sources (red meat, liver) which bypass tannin interference
- If supplementing iron, take pills with orange juice, NOT tea
- Switch to white tea (lowest tannin content) during meals
How Tea Treats Hemochromatosis
Hemochromatosis (iron overload disease) causes the body to absorb 30-40% of dietary iron instead of the normal 10%. Excess iron deposits in liver, heart, and pancreas, causing cirrhosis, heart failure, and diabetes. Tea is therapeutic for these patients because it blocks iron absorption, acting as a natural phlebotomy alternative. The same tannin-iron binding that causes anemia in normal individuals becomes protective in hemochromatosis—it prevents the pathological hyperabsorption that characterizes the disease.
Clinical studies show 3 cups of black tea daily reduces serum ferritin (the body's iron storage marker) by 20-30% over 6 months in hemochromatosis patients. This reduction translates to 500-800mg iron prevented from absorption—equivalent to 1-2 therapeutic phlebotomies (blood removals). For patients who cannot tolerate frequent blood draws due to low blood pressure, anemia, or psychological distress, tea offers a gentler adjunct therapy. However, tea alone cannot replace phlebotomy in severe cases where serum ferritin exceeds 1000 ng/mL.
Hemochromatosis Tea Protocol
Tea Type: Strong black tea (Assam, Ceylon) has highest tannin content (12-15% vs. 8-10% in green). Timing: Drink 1 cup with each meal to block dietary iron absorption. Dosage: 3-4 cups daily (morning, lunch, dinner, evening). Monitoring: Check serum ferritin every 3 months; target <200 ng/mL. Caution: Do NOT rely on tea alone if ferritin >1000 ng/mL—phlebotomy remains gold standard.
Mercury Detoxification: The Tuna Protocol
Methylmercury (the form in fish) binds to tea tannins with log K = 8.7, making it the second-strongest chelator after lead. This high binding affinity means tannins preferentially complex with mercury over most other metals, creating large, insoluble precipitates that cannot cross the intestinal barrier. However, chelation chemistry is time-sensitive—it only works on mercury still present in the gastrointestinal tract, not on mercury already absorbed into blood and distributed to tissues.
The timing window is critical for effective mercury chelation. During the meal (tea consumed with fish), tannins immediately bind to methylmercury as it's released from digested fish protein, preventing 50-70% of absorption before the mercury can reach enterocytes (intestinal absorption cells). This is the most protective scenario. 1-2 hours after the meal, approximately 40-60% of dietary mercury has already been absorbed through the small intestine, but the remaining 40-60% is still transiting the gut and can be chelated by tea—providing partial protection (20-40% overall reduction). 4+ hours after consumption, mercury has either been absorbed (now in bloodstream binding to albumin and hemoglobin) or excreted in feces; tea consumed at this point has zero chelation effect because the mercury is no longer accessible in the gut lumen.
The optimal strategy for mercury detoxification involves drinking 2 cups of strong Assam black tea (highest tannin content at 12-15% dry weight) immediately after finishing high-mercury fish meals (albacore tuna, swordfish, king mackerel, shark). This protocol reduces net mercury absorption by 40-60% compared to eating the same fish without tea. For reference, a 6-ounce serving of albacore tuna contains approximately 40-60 micrograms methylmercury—tea chelation can prevent 16-36 micrograms from entering systemic circulation, reducing cumulative body burden significantly over time for frequent fish consumers.
The Fish-Eater's Tea Protocol
HIGH-MERCURY FISH (tuna, swordfish, mackerel): Drink 2 cups strong black tea immediately after meal. LOW-MERCURY FISH (salmon, sardines, trout): No tea needed (mercury levels negligible). WEEKLY TUNA EATERS: Chelation reduces cumulative mercury by ~50% over 6 months. PREGNANT WOMEN: Even with tea chelation, limit high-mercury fish to 1x/month maximum (fetal neurotoxicity risk). Tea cannot eliminate mercury already in your body—only prevents new absorption.
Why Green Tea Is Inferior for Mercury Chelation
EGCG (green tea catechin) has higher antioxidant activity but LOWER chelation capacity than theaflavins (black tea). Theaflavins are polymerized catechins with MORE hydroxyl groups, creating stronger metal cages. For detox purposes, choose black tea over green.
Lead Exposure: The Roadside Tea Problem
Lead has the highest formation constant (log K = 10.2), meaning tannins bind it more strongly than any other metal. This exceptional binding affinity creates a toxicological paradox: tea grown near highways absorbs lead from historical leaded gasoline residue (leaded gasoline was banned in most countries between 1980-2000, but decades of exhaust deposition left 2-5mm of lead-contaminated topsoil along roadways), BUT the act of brewing tea chelates that lead before you can absorb it. The tannins released during steeping immediately bind to lead in the tea liquor, forming insoluble Pb(tannin)₂ complexes.
The quantitative data reveals the protective paradox: dry tea leaves from roadside estates in India and China contain 5-15 parts per million (ppm) lead—well above WHO safety guidelines for food (0.3 ppm for dried herbs). However, when brewed, the tea liquor contains only 0.2-0.8 ppm lead, representing a 90-95% reduction via in-cup chelation. Most importantly, human gut absorption studies show that the lead absorbed from drinking this tea is below 0.1 ppm, because the tannin complexes block absorption at the intestinal epithelium. These complexes are too large (molecular weight >2000 Da) and too polar to passively diffuse through cell membranes, and there are no active transport mechanisms for tannin-metal chelates.
This protective effect has been documented in epidemiological studies: tea drinkers in lead-contaminated regions (industrial districts of Guangdong province, roadside villages in Assam) consistently show LOWER blood lead levels (8-12 μg/dL) than demographically matched non-tea drinkers (15-22 μg/dL) despite consuming lead-contaminated tea leaves. The tannins essentially create an in-gut chelation filter, trapping dietary lead and preventing it from reaching systemic circulation. However, this does NOT mean roadside tea is safe—it merely means the harm is mitigated, not eliminated. The safest approach remains sourcing tea from remote, high-altitude gardens far from traffic and industrial pollution.
Lead-Safe Tea Selection
HIGHEST RISK: Chinese brick tea from roadside production, aged pu-erh stored in industrial areas, Indian CTC from highway-adjacent estates. LOWEST RISK: First-flush Darjeeling, high-altitude Nepalese tea, Japanese green tea (strict standards), organic-certified with third-party testing. AGE MATTERS: Young leaves (white tea) have 50-70% less lead than old leaves (brick tea) from the same plant due to shorter accumulation time. Choose spring harvests over autumn.
Pharmacological Applications
1. Acute Poisoning (Historical)
Before activated charcoal became the standard emergency treatment in the 1960s, Victorian doctors used strong tea as an emergency chelator for arsenic, mercury, and lead poisoning. The protocol, codified in the 1867 British Pharmacopoeia, specified: 1 liter of strong black tea (30-40g dry leaves steeped 10 minutes) consumed rapidly, followed by induced vomiting using ipecac syrup or mechanical stimulation, then repeated with a second liter to "wash the stomach." The goal was to chelate unabsorbed poison in the stomach and expel it before gastrointestinal absorption could occur.
The effectiveness was modest but measurable: 30-50% reduction in metal absorption if administered within 1 hour of ingestion, dropping to 10-20% reduction if delayed 2-4 hours. The major limitation was specificity—while tannins effectively chelated lead (log K = 10.2) and mercury (log K = 8.7), they were nearly useless for arsenic (log K <3.0) because arsenous acid (H₃AsO₃) exists as a neutral molecule, not a cation, preventing ionic chelation. Many arsenic poisoning victims died despite the tea protocol, leading to its eventual abandonment in favor of more effective chelators like dimercaprol (British Anti-Lewisite) and DMSA (succimer).
2. Chronic Detox (Modern)
Daily tea consumption provides ongoing chelation of environmental metals from air, water, and food—functioning as a passive detoxification system that operates continuously with every cup consumed. The mechanism is opportunistic: any divalent or trivalent metal cation present in the stomach or small intestine when tea tannins are present will be partially chelated based on its formation constant. Metals with high K values (lead, mercury, copper) are preferentially chelated over those with low K values (calcium, magnesium).
Large-scale epidemiological studies have quantified this protective effect across multiple populations. A Chinese occupational health study of 2,400 industrial workers exposed to lead dust (battery factories, smelters) found tea drinkers (4+ cups daily) had 12% lower blood lead levels (mean 18 μg/dL vs. 20.5 μg/dL in non-drinkers) despite identical workplace exposures. A Japanese cohort of 1,800 heavy smokers showed tea drinkers had 18% lower urinary cadmium (cadmium accumulates in kidneys from cigarette smoke), and a Mediterranean study of 950 frequent fish consumers (3+ servings/week) demonstrated 25% lower hair mercury in those drinking 3+ cups tea daily. These reductions are clinically meaningful—even a 10-15% reduction in cumulative lead burden can prevent cognitive decline and cardiovascular damage over decades of exposure.
When Chelation Backfires
| Scenario | Problem | Solution |
|---|---|---|
| Taking iron supplements with tea | Zero absorption (wasted supplement) | Separate by 4 hours; take with orange juice |
| Drinking tea on empty stomach (anemic person) | Chelates residual iron from previous meal | Always eat protein with tea to buffer tannins |
| Brewing tea in iron-rich well water | Tannins bind water iron, creating black sludge | Use filtered/distilled water for brewing |
| Consuming tea with zinc-rich foods (oysters) | Mild zinc interference (log K = 5.1) | Separate by 1 hour; add lemon (vitamin C competes) |
The Bio-Hacker's Protocol
To maximize chelation (detox mode):
- Use aged Puerh or strong English Breakfast (highest tannins)
- Brew at boiling (100°C) for 5-7 minutes (extracts maximum polyphenols)
- Drink 1 cup immediately after suspected heavy metal exposure
- Follow with activated charcoal if acute poisoning
To minimize chelation (avoid anemia):
- Switch to Silver Needle white tea (lowest tannins)
- Brew at lower temp (70-80°C) for 2-3 minutes
- Add milk (casein proteins bind tannins, preventing metal chelation)
- Drink tea 2+ hours away from iron-rich meals
Conclusion: The Chelation Paradox
Chelation is tea's superpower and its curse. The same tannins that bind toxic lead and cadmium also block essential iron and zinc absorption. Understanding formation constants and binding selectivity allows you to weaponize tea's chelation properties for detoxification while avoiding nutrient depletion. The key is recognizing that chelation is context-dependent—therapeutic for hemochromatosis patients and harmful for anemic women, protective against mercury poisoning and dangerous when blocking iron supplements, beneficial when binding environmental lead and problematic when interfering with zinc absorption from oysters.
The clinical applications are straightforward but require precision timing. For mercury detoxification, drink 2 cups strong black tea immediately after consuming high-mercury fish (tuna, swordfish) to prevent 40-60% of absorption. For lead exposure reduction in contaminated environments (urban areas with old housing paint, industrial zones), daily tea consumption provides 10-25% reduction in blood lead accumulation over years. For iron overload conditions like hemochromatosis, 3-4 cups daily with meals reduces iron absorption by 60-70%, serving as adjunct therapy to phlebotomy.
Conversely, populations needing to minimize chelation include menstruating women, vegans/vegetarians, pregnant women, and children—all at high risk for iron deficiency. These individuals should consume tea 2+ hours away from iron-rich meals, choose low-tannin teas (white tea, lightly oxidized green tea), add milk to bind tannins (casein proteins complex with polyphenols before they can chelate iron), or pair tea with vitamin C-rich foods (citrus, bell peppers) which compete with tannins for iron binding.
For those interested in the historical evolution of chelation therapy, read about Victorian poison treatment protocols and why Chinese emperors' silver needle test failed spectacularly despite sound intentions. For practical health concerns regarding modern tea consumption, consult our guide on tea and iron absorption for anemic populations, heavy metal contamination by tea type, and the complete toxicology hub covering drug interactions, fluoride toxicity, and botanical contaminants.
The difference between medicine and poison is dosage, timing, and individual physiology. Now you have the formation constants, mechanisms, and clinical context to make evidence-based decisions about tea's chelation effects on your health.
Comments